DOWNLOAD THIS INFORMATION AS A PDF
Translations – SAMOAN / TONGAN / MAORI / ARABIC / KOREAN
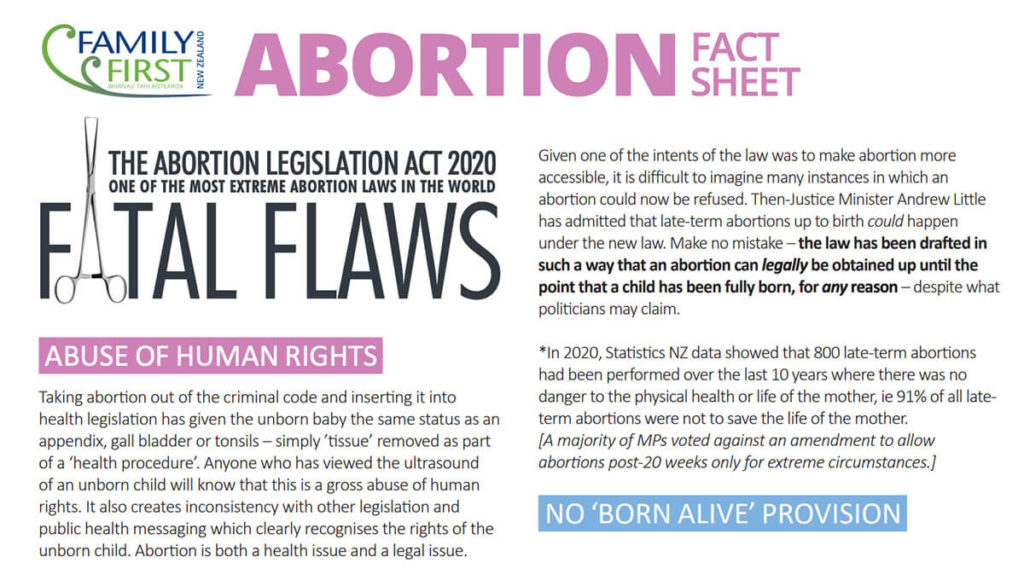
‘FATAL FLAWS’
Abortion Legislation Act 2020
POLICY FAIL
* To remove legislation about abortion from the criminal code and insert it to the health code is to equate a procedure to remove an unborn baby with a procedure to remove an appendix, kidney stones, gall bladder or tonsils – simply ’tissue’ removed as part of a ‘health procedure’. This denies the humanity of the baby and again, creates inconsistency with other legislation and public health messaging which clearly recognises the rights of the unborn child. Anybody who has viewed the ultrasound of an unborn child will know that this policy is a gross abuse of human rights.
 WHEN DOES LIFE BEGIN?
WHEN DOES LIFE BEGIN?
Jacinda Ardern refuses to answer the question put to her by 12 women who have had an abortion and had their full-page Open Letter to the PM published in the major daily newspapers last month. The women asked the PM when does she believe life begins. They say that a failure to answer that question may result in inadvertently killing human beings rather than merely ‘removing human tissue’. The real question we should be debating is at what point does the unborn child become a human being deserving of the same human rights and protections that we all receive and enjoy.
READ: Open Letter to PM Jacinda Ardern
LATE-TERM ABORTIONS UP TO BIRTH ARE LEGAL
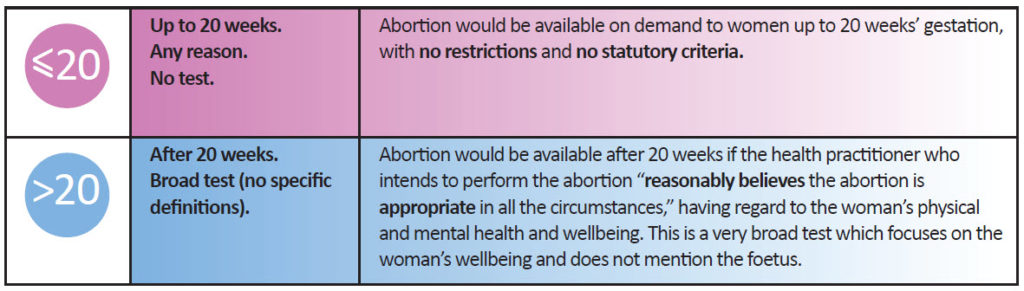
* Late term abortions will increase. Previously the Crimes Act allowed for an abortion after 20 weeks gestation only in exceptional circumstances. Statistics NZ data shows that 800 late term abortions have been performed over the last 10 years where there was no danger to the physical health or life of the mother – 91% of all late term abortions. The new law means that late term abortions will be available to women if the abortion provider “reasonably believes the abortion is clinically appropriate in all the circumstances,” having regard to the woman’s physical and mental health and wellbeing. This is a very broad subjective test.
* for abortions after 20 weeks, the terms “physical health” “mental health” and “wellbeing” are not defined by the Bill. The “gestational age” to be considered is not defined. On a natural reading these terms are broad and unrestrictive. Given the policy intent to make abortion more accessible, it is difficult to see many instances in which an abortion would reasonably be refused. Justice Minister Andrew Little has admitted that late-term abortions up to birth can happen under the new law. A baby could be aborted after 20-weeks as long as the abortionist who intends to perform the abortion considered that the abortion was ‘appropriate in the circumstances’ with a ‘nod’ from a colleague (another abortion provider!). The Bill has been drafted in such a way that an abortion can legally be obtained up until the point that a child has been fully born – irrelevant to what the politicians may promise or claim.
An amendment to allow abortions post-20 weeks ONLY for extreme circumstances was voted against by a majority of MPs.
BORN ALIVE PROVISION VOTED DOWN
* In a shocking display of human rights abuse in New Zealand, an amendment to the Abortion Legislation Bill which required the care of a child born after an attempted abortion was voted against by a majority of MPs. The amendment of National MP Simon O’Connor clarified that a qualified health practitioner who performed an abortion that results in the birth of a child after an attempted abortion has a duty to provide the child with appropriate medical care and treatment, no different than the duty owed to provide medical care and treatment to any other child born. “We should be protecting the lives of innocent babies. We should be making abundantly clear, especially in this abortion legislation, that this is an obligation on medical professionals. Because of international experience here, and here, it was vital to have an express provision in the abortion legislation to reinforce this obligation.
FOETAL PAIN PROVISION VOTED DOWN
An amendment which required the abortion procedures post-20 week to ensure that ‘foetus does not feel pain’ (as per the Animal Welfare Act which requires vets to ensure that animals don’t feel pain!) was voted against by the majority of MPs.
Background: Current guidance for abortions providers in the UK relies on a 2010 review by the Royal College of Obstetricians and Gynaecologists (RCOG) into fetal awareness. In the review the RCOG claims that the unborn baby is in an unconscious state and does not reach consciousness until birth. They have been criticised for this conclusion being based on the evidence from only one paper from 1986, an experiment on sheep foetuses exposed to low oxygen levels. But two medical researchers, including a ‘pro-choice’ British pain expert who used to think there was no chance unborn babies could feel pain before 24-weeks, say recent studies strongly suggest the assumption is incorrect. In an article, published in the influential Journal of Medical Ethics, the researchers say there is now “good evidence” that the brain and nervous system, which start developing at 12 weeks’ gestation, are sufficient enough for the baby to feel pain. They argue that women considering an abortion at this stage of pregnancy should be told about the pain their unborn baby could experience while being terminated.
Currently, the use of pain relief during an abortion in the UK is not required by law or suggested in official guidelines. This in itself is contradicted by the standard NHS practice of giving painkillers to unborn babies receiving surgery in the womb for spina bifida. A UK report recently launched by the All-Party Pro-Life Parliament Group collated evidence on foetal sentience and pain to present to Parliament. Foetal Sentience & Pain: An evidence review, is highly critical of the current RCOG guidelines which permit abortion without analgesia at any gestation, concluding that “The Review has highlighted significant areas of scientific, clinical and philosophical concern, and changes in clinical practice, which should lead the RCOG to review its 2010 guidance.” This report recognises that between 12 and 24 weeks gestation, “There are differing views on which part of the brain controls pain sensations, when foetal pain starts and whether analgesia should be used in the second trimester”, before going to present further evidence to suggest pain may be felt during this period
COERCION & SUPPORT
* No provisions are proposed to protect women and young girls from being coerced into an abortion as a result of abuse or coercion from a boyfriend or family member
* No provisions are proposed for ensuring women have the mental-health support they need before and after abortion, or that women are made fully aware of the risks of abortion, and of all of their options.
The Ministry of Health has even recommended that women should be told that “abortion is safer than continuing a pregnancy”!
NO PARENTAL NOTIFICATION
* There’s no proposal to prevent schools from taking young women for an abortion without parental knowledge. In fact, the new law has removed all safeguards prior to 20 weeks, including for a pregnant child who could access an abortion on demand. A young teen could simply self-refer without any safeguards. In all other health contexts, the health practitioner is required to assess the child’s capacity prior to a medical procedure and, where capacity is lacking, obtain the consent of a parent or guardian. Why can parents be deliberately excluded from this procedure? It is ironic that abortion supporters want abortion to be treated as a ‘health’ issue – but not when it involves a teenager! An amendment for parental involvement and for abortion for minors to be treated like other health procedures was voted against by a majority of MPs.
FREEDOM OF CONSCIENCE PROVISIONS
* The law also waters down the freedom of conscience rights for health practitioners, who would be required to provide information to women about abortion service providers. The effect of the ability for an employer to refuse to hire someone, or to terminate their employment, on the grounds of their conscientious objection is concerning. Amendments to keep conscientious objection standards the same as they currently are (the bill currently weakens the protections) were voted against by the majority of MPs.
SEX SELECTIVE ABORTIONS
 * There’s no proposal to specifically prevent sex-selective abortion, except for a ‘tut-tut-tut we don’t like it’ provision. Sex selective abortion is a well-known problem in China and India, where son-preference cultures have resulted in extremely skewed sex ratios. Sex discrimination carried out via abortion is well documented and has resulted in millions of “missing” girls in some societies. The number of girls and women missing from the global population is estimated to be more than 160 million, with sex selection being a major culprit. The practice of sex selection has been widely condemned.
* There’s no proposal to specifically prevent sex-selective abortion, except for a ‘tut-tut-tut we don’t like it’ provision. Sex selective abortion is a well-known problem in China and India, where son-preference cultures have resulted in extremely skewed sex ratios. Sex discrimination carried out via abortion is well documented and has resulted in millions of “missing” girls in some societies. The number of girls and women missing from the global population is estimated to be more than 160 million, with sex selection being a major culprit. The practice of sex selection has been widely condemned.
There is evidence that sex selective abortion is already occurring in some parts of Australia – for example, the high-profile case of Dr Mark Hobart who refused to perform a sex-selective abortion in Victoria, or the investigation by SBS that found a higher number of boys than girls being born in some ethnic communities in Australia. New Zealanders are resolutely opposed to sex-selection abortions. In polling released at the beginning of the year, it found that 90% oppose sex selective abortions – only 4% support. Women are 94% opposed, and 91% of those who generally support abortion are opposed. It is definitely a crime when baby girls are being aborted simply because they’re baby girls. An amendment to place an explicit ban on sex selection abortions was voted against by a majority of MPs.
DANGEROUS D.I.Y. ABORTIONS AT HOME
 * Women may now be able to access dangerous DIY abortions at home, and possibly even school. Previously, abortions could only be performed in licenced institutions. Under the new extreme law, the requirement that abortions take place in a licensed institution has been removed. Under the new policy, a single doctor is able to prescribe abortion pills over the phone or video (eg Facetime, Zoom or Skype) and then women will perform their own abortion at home by taking both abortion pills, meaning they will be left to pass their unborn child at home without direct medical supervision.
* Women may now be able to access dangerous DIY abortions at home, and possibly even school. Previously, abortions could only be performed in licenced institutions. Under the new extreme law, the requirement that abortions take place in a licensed institution has been removed. Under the new policy, a single doctor is able to prescribe abortion pills over the phone or video (eg Facetime, Zoom or Skype) and then women will perform their own abortion at home by taking both abortion pills, meaning they will be left to pass their unborn child at home without direct medical supervision.
* In practice, it would be possible that abortions could be available in thousands of locations in communities across New Zealand including sexual health clinics, GPs’ surgeries, school nurse clinics, university health clinics, and possibly even mobile abortion clinics. When self-administering pills are delivered to the home by a courier company, there is no control over who takes the pills, when the pills are taken, whether the pills are taken, if the woman or girl is vulnerable or in an abusive or coercive relationship, and if another competent adult is present. All of this will place women at risk. The removal of any direct medical supervision overseeing the use of both abortion pills could see a rise of complications experienced by women, with possibly no-one present to assist her in a medical emergency. It would be easier for third parties to obtain abortion pills and slip them into a woman’s food without her knowledge. It also poses a threat to vulnerable girls who are at risk from sex-trafficking or child-sex abuse, as the ‘home’ abortion could be used by their abusers as a means to more easily cover up trafficking or abuse scandals. Parents should also be concerned that abortions could potentially happen at schools. READ MORE
LOOSE DEFINITION OF ‘HEALTH PRACTITIONER’
* There is no requirement in the new law that the Qualified Health Practitioner who provides abortion services, at any point in a woman’s pregnancy, is a doctor. In fact, the Bill specifically uses the term “Health Practitioner” rather than “Medical Practitioner” thereby broadening the category of person empowered to certify and carry out abortions beyond just doctors
 GESTATIONAL TIME LIMIT FOR DISABILITIES
GESTATIONAL TIME LIMIT FOR DISABILITIES
* The new law has also removed the current 20-week gestational time limit for disability. Jacinda Ardern has also betrayed her promise to the Down syndrome community. In 2017 during the election campaign, the organisation Saving Down’s highlighted their concerns around Jacinda Ardern’s pledge to change abortion laws, saying that this would introduce abortion through to birth for babies with disabilities. In response, Jacinda Ardern made a commitment to not increase the time limit for disability-selective abortion. In the UK, there are increasing numbers of late term abortions for conditions such as such as cleft lip and palate or club foot. An explicit ban on disability discrimination abortions was voted against by a majority of MPs. READ MORE
 PUBLIC OPPOSITION
PUBLIC OPPOSITION
* more than 90% of submissions opposed the bill
* almost 95% of submitters who wanted to speak to the committee were denied
* polling has found that only 4% of New Zealanders want more liberal time limits for abortion
* polling last year found strong support for the unborn child having human rights and being legally protected once a heartbeat is detected – which can be between 6–12 weeks – and only a small minority thinking that life doesn’t begin until the child is born
VOTING RECORD
CLICK HERE to see who voted for (and against) the bill
 AMENDMENTS (all voted down)
AMENDMENTS (all voted down)
When the abortion bill was looking likely to pass (as was always likely with the current parliament that we have), attempts were made by pro-life MPs during the Committee stage to ‘soften’ the harms of the bill and to take the extreme aspects away from this flawed bill.
The proposed amendments were all defeated (and are recorded in our voting record sheet in order of the list below):
- BORN ALIVE: requirement that a qualified health practitioner who performed an abortion that results in the birth of a child after an attempted abortion has a duty to provide the child with appropriate medical care and treatment, no different than the duty owed to provide medical care and treatment to any other child born.
- SEX SELECTION: explicit ban on sex selection abortions which do happen both here and and overseas
- DISABILITY: explicit ban on disability discrimination abortions
- PARENTS: parental involvement – abortion for minors treated like other health procedures.
- FOETAL PAIN: requirement for abortion procedures post-20 week to ensure that foetus does not feel pain (as per the Animal Welfare Act which requires vets to ensure that animals don’t feel pain!)
- LATE TERM: abortions post-20 weeks only for extreme circumstances
- CONSCIENCE: keeping conscientious objection standards the same as they currently are (the bill currently weakens the protections)
- REFERENDUM: a referendum so that we all get a say on this crucial issue, similar to euthanasia
CLICK HERE to see the summary of how each MP voted
Or click on images below to download PDF version of voting record

FURTHER BACKGROUND INFORMATION
** Please note – this is information that was provided before the new extreme law was passed in 2020 **

CURRENT ABORTION LAW
What is the current abortion law in New Zealand?
Under the Crimes Act 1961, it is a crime to perform an abortion unlawfully, or to supply the means of providing an abortion (such as drugs or instruments) unlawfully (ss. 183 and 186). Women are explicitly exempt from liability, meaning a woman cannot be criminally charged for having an abortion under the Crimes Act 1961. However, under s.44 of the Contraception, Sterilisation and Abortion Act 1977, it is a crime for a woman to receive an abortion unlawfully. Thus, performing, receiving or supplying the means of providing an abortion is a crime only when it is not carried out in accordance with the proper procedure and legal criteria for lawful abortions.
What are the criteria for a lawful abortion?
In the case of a pregnancy of not more than 20 weeks’ gestation, a lawful abortion may be performed if one of the following criteria are met:
- Serious danger to the woman’s life, physical or mental health (factors which may also be taken into account: the woman’s age, and whether the pregnancy is the result of sexual violation); or
- Foetal abnormality (a substantial risk that the baby will be “seriously handicapped”); or
- The pregnancy resulted from incest or sexual intercourse with a dependent family member; or
- The woman is “severely subnormal” (has a mental, physical or intellectual impairment that significantly impairs her ability to understand and make decisions about sexual conduct).
(Crimes Act 1961, s.187A(1))
In the case of a pregnancy of more than 20 weeks’ gestation, a lawful abortion may be performed only when it is necessary to save the woman’s life, or prevent serious permanent injury to her physical or mental health.
(Crimes Act 1961, s.187A(3))
Are women currently ‘criminalised’ for having abortions in New Zealand?
No. Under the Contraception, Sterilisation and Abortion Act 1977, it is a crime for a woman to receive an unlawful [i] abortion in New Zealand (for example, a ‘backstreet’ abortion). This offence creates some individual responsibility for women who attempt to bypass the proper criteria and procedure for lawful abortions (albeit with a relatively low penalty of a maximum fine of $200). Importantly, since 1977 when the current law was enacted, the Ministry of Justice has no record of any woman ever being convicted for receiving an unlawful abortion. It is therefore wrong to say that women are ‘criminalised’ for receiving abortions under the current law.
Who then is ‘criminalised’ under New Zealand’s current abortion laws?
According to the Law Commission, there is no record of any case in which a person has been convicted for performing an unlawful abortion. There has been a small number of convictions under s. 183 for procuring (i.e., performing) an unlawful abortion. However, Ministry of Justice records show that these related to physical assaults on pregnant women that caused (or were intended to cause) a miscarriage – not medical or surgical abortions. There has been one conviction for providing the means of procuring an unlawful abortion (for supplying pills illegally).
Does New Zealand have ‘abortion on demand’?
Not officially. By law, there is no automatic ‘right’ to have an abortion. However, in practice, there is evidence to suggest that abortion is more accessible than the law would appear to allow, because certifying Consultants adopt a very wide interpretation of the ‘mental health’ ground for abortion. Most abortions are provided on this ground. New Zealand’s annual abortion rate is comparable to jurisdictions with ‘health’-oriented abortion laws, which may suggest that a high percentage of requests for abortion are granted.
Former Chair of the Abortion Supervisory Committee, Dr Christine Forster, said, “We do essentially have abortion on demand or request, however you like to put it. […] Certainly in the main centres, in Auckland, Wellington and Christchurch, if a woman wants an abortion I think she’ll get one.” [ii] The Hon Judith Collins has stated in Parliament, “To be absolutely frank, we have abortion on demand in New Zealand, in everything except name.” [iii]
PROPOSED ABORTION LAW
What changes are proposed to abortion law?
The Government has proposed a policy shift to treat abortion as a ‘health’ issue rather than a criminal issue. This would involve removing the criminal offences regarding abortion and treating abortion like other health services, which are governed by general health laws and professional guidance.
Why does the Government want to reform abortion law?
The focus of this policy shift is entirely on the ‘wellbeing’ of women seeking abortion. The Government seeks to remove the element of censure that the criminal law entails, and to make abortion more accessible, with fewer delays. The Government does not appear to have considered the status of a foetus, nor any State interests in preserving life. Under the current law (Crimes Act 1961), an unborn child is afforded some recognition and (minimal) legal protection. In contrast, treating abortion as a health issue and removing it from the Crimes Act 1961 gives the unborn child the same status as an appendix, tonsils or gall bladder – simply tissue removed as part of a ‘health procedure’.
What would a new abortion law permit?
Does this mean late-term abortions will become legal?
‘Late-term abortion’ is a term used to describe abortions from the second trimester of pregnancy onward. Some use this term for abortions performed from 16 weeks (including the Law Commission), and others use it for abortions performed after 23 weeks (related to viability). Late-term abortions are already legal in some circumstances (see para 3 on previous page), and data provided by Statistics NZ shows that that more than 850 late term abortions have been performed over the last 10 years where there was no danger to the physical health or life of the mother.
The Abortion Legislation Bill would make late term abortions considerably more accessible than they are under the current law. After 20 weeks’ gestation, a baby could be aborted as long as the health practitioner who intends to perform the abortion considered that the abortion was ‘appropriate in the circumstances’.
What do the proposed models for abortion law reform leave out?
The Abortion Legislation Bill leaves serious gaps. No provisions are proposed to protect women from being coerced into an abortion. No provisions are proposed for ensuring women have the mental-health support they need before and after abortion, or that women are made fully aware of the risks of abortion, and of all of their options. There’s no proposal to prevent schools from taking young women for an abortion without parental knowledge, or to prevent sex-selective abortion. The Bill also waters down the freedom of conscience rights for health practitioners, who would be required to provide information to women about abortion service providers. It is proposed that employers could terminate a health practitioner’s employment, refuse to employ a new job applicant, or offer health practitioners less favourable terms of employment, conditions of work, or opportunities for training if the employee’s or job applicant’s conscientious objection to abortion would “unreasonably disrupt the employer’s activities”.
The bill would also remove the current 20-week gestational time limit for disability. Instead, abortion will be available for disabilities including Down syndrome right through to birth, providing one registered health practitioner signs off on the abortion under the new ‘well-being’ grounds. In the handful of jurisdictions that have similar laws, this has in practice allowed for abortion for disabilities including Down syndrome right through to birth. In 2017, the organisation Saving Down’s highlighted their concerns around Jacinda Ardern’s pledge to change abortion laws, saying that this would introduce abortion through to birth for babies with disabilities. In response, Jacinda Ardern made a commitment to not increase the time limit for disability-selective abortion.
DOWNLOAD a more detailed examination of the bill.

‘Changing the law is simply ratifying what’s already happening’
What is being proposed is not simply a case of ratifying current practice. Instead it would attempt to introduce a new and extreme abortion law in NZ – a law that could result in the removal of safeguards for women, the introduction of late-term abortion, the loss of freedom of conscience forhealthcare providers, and gender- selective abortions, among other things.
‘Women who have abortions shouldn’t be criminals’
This claim is simply false scaremongering aimed atdeceiving people into supporting the introduction of an extreme abortion law in New Zealand. Any New Zealand woman who has an abortion under the current legislative guidelines and protections is notcommitting an illegal act and is therefore notconsidered a criminal by our current laws. Women are not made criminals by the current legislative guidelines and protections. The existing safeguards are there to protectwomen from unlicensed premises and coercion, and it is these safeguards most New Zealanders support.
‘There is no point in keeping abortion in the Crimes Act, it’s a health issue’
The current law recognises the scientific fact that there are at least two human beings involved in every pregnancy, and that abortion results in the loss of one of those lives. The current legal framework attempts to strike a balance between the wellbeing of the mother, and the fact that the deliberate taking of any innocent human life is a crime that must be safeguarded against.
And yes, abortion is also a health issue – it’s a surgical procedure that has some serious risk factors associated with it. A sound law needs to reflect that reality, and notleave women exposed to harms, such as those recently witnessed in the criminal trial of US abortionist Kermit Gosnell who was able to operate a dangerous but legal abortion facility which resulted in female client death and other atrocities thanks to extreme abortion laws. Criminal consequences for abortion providers who break the law should remain, in order to better protect all the parties involved.
 ‘It’s a matter between a woman and her doctor’
‘It’s a matter between a woman and her doctor’
There are at least two human beings involved in every pregnancy, and that’s why we place such a strong emphasis oncampaigns which discourage smoking or drinking during pregnancy in this country. It’s also why, if it is needed, doctors conduct life-saving surgery while a child is in utero.
Any responsible doctor knows that they are dealing with at least two patients that need care every time a pregnant woman comes under their supervision, and any responsible law should also do the same.
‘Women currently have to jump through hoops to get an abortion’
The system currently puts basic legal safeguards in place. Even the Abortion Supervisory Committee (ASC), in its latest reportto Parliament, notes that, “The ASC recognises the merit in having a robust pathway in place, which requires certifying consultants to assess and certify patients and to ensure counselling is offered.” If there truly are issues with these current safeguards, then addressing those areas, and not introducing an extreme abortion law, is the correctway to fix any deficiencies.
‘Women must have control over their own bodies’
New Zealand women need to be informed of the effects that abortion can have on their bodies, and the current law needs to be strengthened to ensure that informed consent from an independent provider is a legal requirement.
There are at least two bodies in every pregnancy: the body of the mother and the body of the unborn human being. If we truly believe that women must have control over their bodies, then surely unborn women deserve the right to their bodies too?
 ‘Women deserve the right to choose’
‘Women deserve the right to choose’
Yes, all women deserve the right to choose, including the unborn little girl’s right to grow up and make choices.
Women should have the right to choose – their maternity care provider, their midwife, their doctor, the type of birth they want, etc – but abortion is something completely different altogether. Abortion is the choice to end the life of another human being.
The question of choice is far more complex than the way it is often portrayed in the abortion debate. The law, in general, doesn’t recognise personal choice as an absolute without limits; it always restricts choice when it conflicts with the wellbeing of others. In the case of abortion, those ‘others’ are the unborn human beings who will be robbed of ALL their choices if they are aborted.
A real choice is one that is fully informed; about all the risks, about all the options, about foetal development, and about what the abortion procedure actually entails.
‘Private decisions like abortion shouldn’t be the government’s business’
All of us have a stake in what happens to the most vulnerable members of our community and to their mothers, so we should all care about what shape our laws take when it comes to abortion.
‘Every child needs to be loved and wanted’
Children need to be accepted and loved because they are valuable, regardless of whether or not they were ‘planned’. A so-called ‘wanted child’ is no more special or valuable than a child that has parents who are too afraid or unsure to ‘want’ that child right now. The ultimate act of love is to give life to a child. There is also no shortage of loving Kiwi couples who would jump at the chance to adopt and love any so-called ‘unwanted children’ in this country.
‘What about cases of pregnancy resulting from rape or incest or where there are foetal abnormalities?’
Extreme violence has been committed against any woman pregnant from rape or incest. They deserve to be treated with the deepest compassion and given enormous support and care.
However, the circumstances of the baby’s conception change nothing about the baby herself, or the violent nature of abortion. So often when this issue is raised, people refer to the unborn child as if she is an extension of the rapist, or his vile act, completely forgetting that in actual fact the child is her own unique person quite independently of the tragic circumstances of her conception. The child is just as much an extension of the mother. Adding abortion after rape simply adds violence to violence, creating a second victim of the rapist – the unborn child.
Many women who have kept a child conceived in rape tell a common story of finding a silver lining of love in an otherwise very dark situation. Women who keep their babies also avoid the serious psychological risks associated with abortion, which, according to some experts, could be amplified even further when added to the already horrific trauma of sexual assault.
‘What about cases of foetal abnormalities?’
Aborting a child because of possible abnormality is nothing less than blatant discrimination against people with disabilities. When reflecting on this argument we need to tear aside the veil of prejudice that drives the notion that it is somehow kinder to kill a person with a disability or a disease before she is born than to let her ‘live in that condition.’ Shockingly, the types of disabilities included by pro-abortionists in the list of purportedly ‘good reasons’ for an abortion range from the truly severe to relatively minor; the latter part of the list grows lengthier every year. Abortion is becoming a search-and-destroy method for eliminating less-than-perfect people.
In jurisdictions that have decriminalised abortion – China, Vietnam, Canada and two states in Australia – gestational time limits for disability-selective abortions have been removed and abortion for babies with disabilities is available right up to birth. The report on Iceland and their near 100% abortion rate from Down syndrome has led to global controversy regarding equality and non-discrimination for people with disabilities.
Women have a right to be fully informed
A just-published research review paper “Abortion and the Physical and Mental Health of Women – A review of the evidence for health professionals” reviews the international evidence to date about the relationship between abortion and the physical and mental health of women. It shows that abortion is associated with a wide range of adverse physical and psychological outcomes, and it is essential that women are made fully aware of all the risks. It concludes that while studies on abortion have sometimes yielded inconsistent results, there is a clear correlation between abortion and adverse psychological outcomes.
Other conclusions based on the research analysis include:
- Intimate partner violence (IPV) is strongly correlated with abortion, with some research showing a 6-fold increase of IPV in women undergoing abortion compared to those in antenatal care. Abortion has also been linked to international trafficking and slavery of women. Presentation for abortion may be an opportunity to address the risk of coercion and intimate partner violence.
- Ambivalence to abortion is common and is linked to some adverse post-abortion outcomes.
- The prevalence of foetal abnormalities has increased in many countries. Women commonly report a lack of information provided to them about the child’s condition and the options open to them (an example was covered recently in the NZ media).
- The physical effects of abortion include an increased risk of premature delivery in subsequent pregnancies. This appears to be related to surgical abortion but not medical abortion.
- Significant inconsistencies exist in research about a possible link between abortion and the risk of breast cancer, yet there is evidence showing that carrying a pregnancy to term is protective against breast cancer.
The research paper includes NZ-based studies including the University of Otago study in 2008 which found that women who had an abortion faced a 30% increase in the risk of developing common mental health problems such as depression and anxiety. And a research paper entitled “Does abortion reduce the mental health risks of unwanted or unintended pregnancy? Are-appraisal of the evidence” by Professor David Fergusson, John Horwood, and Joseph Boden, published in the 2013 edition of the Australian and New Zealand Journal of Psychiatry, concluded that abortion was not associated with a reduction in rates of mental health problems, but was associated with increases in risks of anxiety, alcohol and drug misuse, and suicidal behaviour. They state: “There is no available evidence to suggest that abortion has therapeutic effects in reducing the mental health risks of unwanted or unintended pregnancy. There is suggestive evidence that abortion may be associated with small to moderate increases in risks of some mental health problems.”
Women deserve to know this information so they can make a truly informed decision, as they should with any health decision.
Abortion numbers are dropping – that’s a good thing!
Everyone is welcoming the drop in the number of abortions – the lowest rate in over 25 years.
The rate will continue to drop as knowledge of the prenatal development of the unborn child increases, and as an increasingly pro-life younger generation become parents themselves.
The ‘bunch of cells’ argument which has driven the right-to-abortion argument is simply flat- earth science. 3-D ultrasounds and smartphone apps allowing parents to listen to the heartbeat of their unborn child and keep track of their baby’s progress in the womb, including heartbeats per minute, the number of times the baby kicks and the weight of the growing foetus, have contributed to an increasing awareness of the life of the child in the womb.
An open letter to the Prime Minister from women who have had abortions
click on image to download PDF
What do New Zealanders really think?

DOWNLOAD Family First’s Submission DOWNLOAD Family First’s Oral Submission WATCH Family First’s Oral Submission