The time following a declined assisted dying application is one of heightened mental health risk, says psychiatrist and University of Auckland senior lecturer Gary Cheung. Patients who request assisted dying are at a higher risk of suicidal thoughts, Dr Cheung told a GP CME audience in Rotorua last month. A 79-year-old with pancreatic cancer, who lived alone and had very little independence, was the first case study.
The patient contacted his GP and enquired about assisted dying, but he did not meet the criteria because his condition was not deemed irreversible. The man went home and attempted suicide twice before health professionals followed up and organised a mental health referral and respite care in a resthome.
The second case was a 96-year-old who had recently lost his wife. Despite having no chronic illness, he applied for assisted dying, and was denied. Shortly after, the man was lonely and desperate, and attempted suicide. He was moved into residential care and prescribed antidepressant medication.
The denial of both these requests was justified in that neither patient met the criteria, Dr Cheung says, but the patients’ GPs needed to act more quickly to connect them with mental health services. The Assisted Dying Service, at the Ministry of Health, has a range of resources – such as Responding when a person raises assisted dying: a handbook for registered health professionals – as well as clinical advisors who can help guide health professionals.
Rules govern the conversations health practitioners may have on the topic. For example, they are not allowed to recommend or even bring up the idea of assisted dying. The request must come from the patient. Doctors are allowed to make a conscientious objection in responding to an assisted dying request, but there are processes that must be followed so the patient can receive the care elsewhere.
“You can choose to not be involved in [the assisted dying process], you can object,” says Dr Cheung. “But you are required to respond to the request. You must inform the patient of a new practitioner who can assist them.” He has heard of many practitioners ignoring requests from patients. Dr Cheung has been a psychiatrist for 20 years and is also a suicide prevention researcher. He notes the End of Life Choice Act 2019 took effect in November 2021 – “it’s still early days, and we’re still learning”.
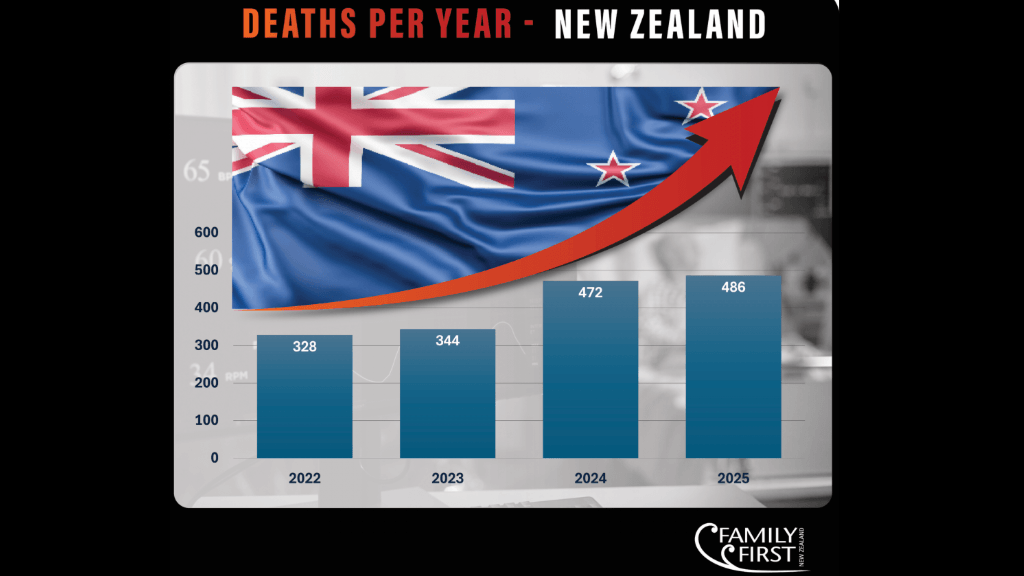
Delegates at the 20-minute presentation filled the conference’s main plenary room, reflecting his point that, while the number of assisted deaths has so far been low, it is increasing and GPs are desperate to be prepared.
The Assisted Dying Service has received 661 applications, and these translated into 257 deaths:
- 80 per cent of the deaths were Pākehā people, 5.5 per cent were Māori
- 55.2 per cent were female patients
- 77 per cent were already receiving palliative care, and
- 67 per cent were cancer patients.
The experience of Australia indicates that the number may increase with time, Dr Cheung says.
To be eligible for assisted dying, a person must meet all of the following criteria:
- be aged 18 years or over
- be a citizen or permanent resident of New Zealand
- suffer from a terminal illness that is likely to end their life within six months u be in an advanced state of irreversible decline in physical capability
- experience unbearable suffering that cannot be relieved in a manner that the person considers tolerable, and
- be competent to make an informed decision about assisted dying.
Originally published at Right to die may be deeply felt: Following a denied application, a patient’s mental health is often at risk | New Zealand Doctor (nzdoctor.co.nz)