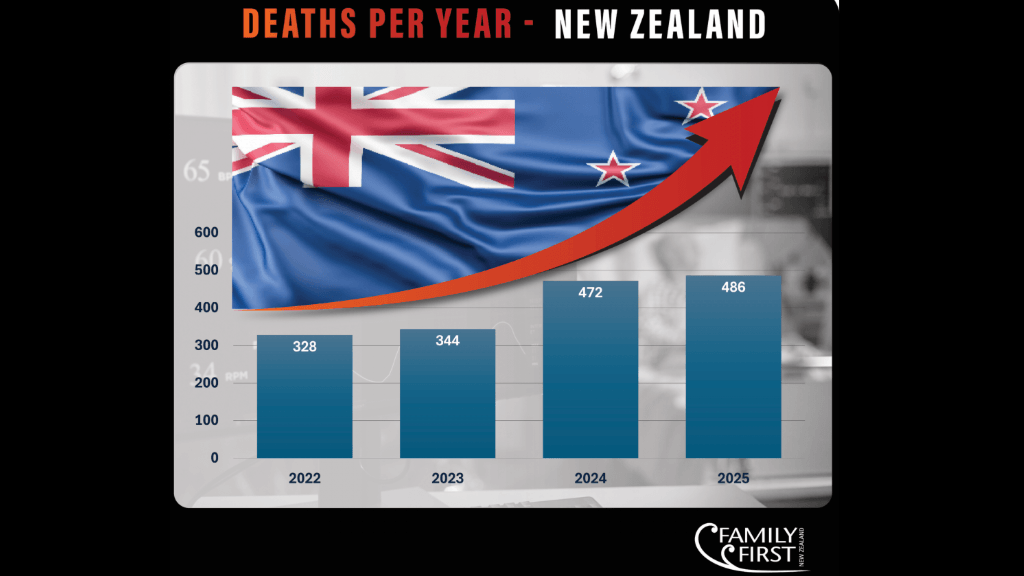
New Zealand’s Registrar of Assisted Dying has just released the fifth annual report on the End of Life Choice Act, and the headline figure is striking: 486 people died by assisted suicide between April 2025 and March 2026, up from just 66 in the law’s first partial year — a roughly sevenfold increase in five years. Applications for the service grew by a further 13% in the most recent year alone. On the surface, this looks like a service settling into steady, orderly operation. Look more closely at the Registrar’s own data, however, and a more troubling picture emerges: a system expanding faster than its safeguards can be meaningfully tested, serving a population that is disproportionately old, ill and already dependent on care, while the oversight body tasked with reviewing every death has received no compliance recommendations at all.
The numbers at a glance
- 1,289 applications were active during the year (1,164 new, plus 125 carried over) — a 13% increase on the previous year
- 306 applications (24%) ended because the applicant died from their underlying illness before the process concluded
- 42 people (3%) withdrew their application
- 486 people (38% of active applications) had an assisted death
- 94.4% of assisted deaths were by injection, administered by an attending medical or nurse practitioner (AMP/ANP)
- The number of assisted deaths represented 1.29% of all deaths in New Zealand during the period
Double-digit annual growth in applications looks less like a rare and carefully guarded choice and more like the gradual normalisation that pro-life advocates have long warned about. The Registrar’s own report concedes that the level of public detail it can share remains limited “while numbers remain low”, but with hundreds of assisted suicide deaths now occurring annually, that justification is wearing thin.
Transparency has not kept pace with volume. Even the workforce has not kept up with the increased numbers. Only 121 practitioners nationwide are currently on the SCENZ Group lists — the register of health professionals willing to provide assisted dying services. Following a review this year, the list shrank, even as applications rose by 13%.
Who is dying
The demographic data in this report require close attention. Eighty percent of applicants were aged 65 or older, and 80% were already receiving palliative care when they applied. In other words, this is not a population making a clear-eyed choice from a position of independence and strength. It is a population already in deep physical decline, often dependent on others for daily care — precisely the group most likely to feel, consciously or not, that they have become a burden.
The report indicates that 6.53% of applicants reported having a disability. International disability rights advocates have voiced concerns for years, noting that assisted suicide frameworks, despite their intentions, can subtly pressure vulnerable groups like the elderly, ill, or dependent. Even when no coercion is intended, framing such decisions around “choice” for individuals constrained by health and dependency raises questions about the true level of autonomy involved.
Are the safeguards real, or just paperwork?
The most notable point in the report is that the End of Life Review Committee, tasked with assessing each assisted death for compliance, made no recommendations on compliance issues during the entire reporting period. Out of 486 deaths, this committee did not identify any problems. This raises the question: does this indicate a perfectly functioning system, or does it suggest that the review process isn’t sufficiently thorough in its search for issues?
Consider, too, the eligibility standard applicants must meet: “unbearable suffering that cannot be relieved in a manner the person considers tolerable.” This is not an objective clinical threshold — it is defined by the applicant’s own perception. Presented as a strict safeguard, it functions in practice as a soft and subjective one.
The report notes that no suspected cases of coercion were identified during the reporting period. However, relying on practitioner judgment and self-report in a limited number of consultations makes it unlikely to detect subtle pressures (such as financial, emotional, or familial) that often do not openly reveal themselves. Zero detected cases do not necessarily mean no cases exist.
Palliative care needs more attention
Buried in the report is perhaps its most important admission: some applicants who began the assisted suicide process withdrew after being connected with “optimised palliative care or additional social or wrap-around supports.” This continues to raise the question critics of the End of Life Choice Act have long asked: is New Zealand responding to gaps in its palliative care system by offering a pathway to death, rather than by funding the care that might have changed people’s minds? If better-resourced palliative and social support can reliably persuade people to withdraw their applications, is that not sufficient evidence to invest in palliative care as a first response, rather than as a backstop offered only after someone has already begun the assisted suicide process?
Complaints
The Act is explicit: only the patient can raise the option of assisted suicide. A health practitioner is not permitted to bring it up unprompted. Yet the report itself documents a complaint to the Health and Disability Commissioner in which a counsellor reportedly raised assisted dying options with a patient who had come in about pain management. This is not a hypothetical scenario; this is a recorded case in the Registrar’s report, and it remained unresolved at the time of publication. If this core safeguard can already be breached within five years of the law’s operation, its long-term reliability deserves serious scrutiny.
Two separate complaints to the Health and Disability Commissioner cited a lack of support for bereaved families. The Act’s framework centres entirely on the individual’s choice to die, but the report shows no equivalent infrastructure for the families who live with the aftermath. If anything, this underscores a law that prioritises the individual’s choice over the well-being of those left behind.
Differences in ethnicity data point to differences in values
The report shows that 81% of applicants identify as New Zealand European/Pākehā, compared with 5% Māori, 2% Asian, and 13% Other. This gap is often framed by the pro-choice camp as an equity and access problem to be solved. Yet a persistent gap like this points to an explanation that is constantly overlooked by politicians and even policymakers. Perhaps the lower Māori uptake isn’t a barrier to be removed; rather, it reflects differences in cultural values and views on the sanctity of life that policymakers and even politicians should listen to, rather than work to override. This kind of disparity in the uptake of a life-ending procedure isn’t a problem to be fixed either. It is a reminder that many New Zealanders still value life and choose to share in the palliative care of their loved ones who are suffering.
Conclusion
This report should trouble every New Zealander who cares about how we treat our most vulnerable. Behind the statistics are 486 real people — mothers, fathers, grandparents — whose lives ended not because our society had exhausted every way to care for them, but because, in too many cases, palliative care options never reached them in time. That is not compassion. That is a failure of care dressed up as choice.
A compassionate society does not respond to suffering by helping people die faster. It walks alongside them and invests in world-class palliative care. The fact that some applicants withdrew once they were finally offered proper support tells us everything we need to know: people do not want to die. They want to be cared for, yet too often they are not.
This report also quietly exposes serious issues: a safeguard has been breached, a review committee has not raised any concerns in a whole year of monitoring hundreds of deaths, and a law claiming to keep things rare, controlled, and watched is being challenged by the very data supposed to reassure us. Every family should be able to trust that their vulnerable loved ones are protected, not merely managed.
New Zealand does not need an increased assisted suicide industry or a broader scope of the End of Life Choice Act. Instead, it needs a national recommitment to and investment in palliative care, strengthening family and community support, and a cultural shift that recognises the worth and dignity of every life, particularly when it is vulnerable. The true test of a compassionate nation is not how swiftly it facilitates death under the guise of choice, but how well it cares for its people until the very last moment.
Source: Ministry of Health. 2026. Assisted Dying Service – Ngā Ratonga Mate Whakaahuru: Registrar (assisted dying) Annual Report to the Minister of Health – June 2026. Wellington: Ministry of Health.